|
Should
we be teaching single
rescuer procedure as the
first line action for
adult cardiac arrest?
Well, we think the
answer is no. Current
assessment requirements
for CPR and First Aid
training in Australia
require the following:
-
perform
uninterrupted CPR on
both an adult and an
infant resuscitation
manikin placed on
the floor
-
use
correct hand
location,
compression depth
rate in line with
the ARC recommended
ratio of
compressions and
ventilations
-
follow single
rescuer procedure,
including the
demonstration of a
rotation of
operators with
minimal
interruptions to
compressions
Some
would say, what’s wrong
with this requirement?
Firstly,
there is no requirement
for this is only
done in Advanced classes
which are rarely
delivered in workplaces.
We need
to go back to basics to
be able to understand
the inefficiency of
single rescuer CPR.
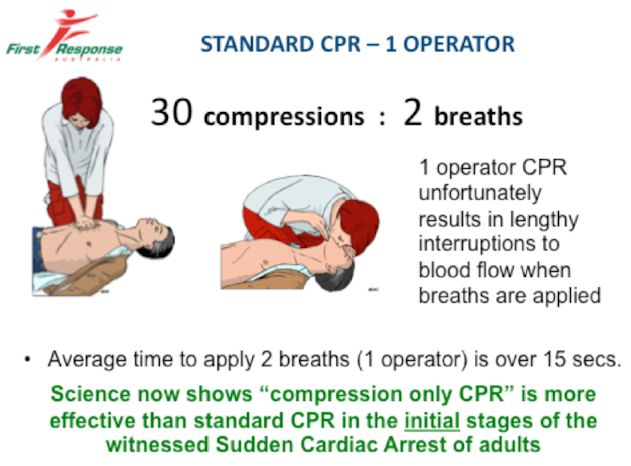
The
recommended ratio of
compressions to breaths
is 30:2. This results in
only 30% of the
resuscitation time being
spent doing
compressions. The
scientific evidence
demonstrates clearly
that to increase
survivability with CPR
there needs to be over
80% of the time doing
compressions. This is
call compression
fraction! – the
percentage of time doing
compressions.
Now don’t
forget, lay people only
practice CPR when they
attend a training
course, which is
possibly only once a
year and then only
spending a few short
minutes (maybe only up
to 5 minutes, actually
doing CPR).
If we
look at the maths, it
goes like this:
It takes
approximately 20 seconds
to do 30 compressions,
then it takes an
additional 15 seconds to
complete the 2 breaths
(and we are assuming
here, that the breaths
have been successfully
delivered and with in
all honestly, breaths
almost never work and
additional time is spent
attempting to redo the
breaths, consuming even
more time). Then we’re
back to the next cycle.
So now to
complete 1 cycle of 30:2
probably takes in the
real world about 30
seconds plus and the end
result being that
possible 2-3 breaths
have been delivered per
minute and only 50-60%
of the time spent doing
compressions. Because of
the lengthy time
interrupting
compressions the amount
of effective forward
blood flow is minimal.
Now add
the time it takes to
utilize a defibrillator
which is approximately
25 seconds plus every 2
minutes, we now only
have a compression
fraction of maybe 50%
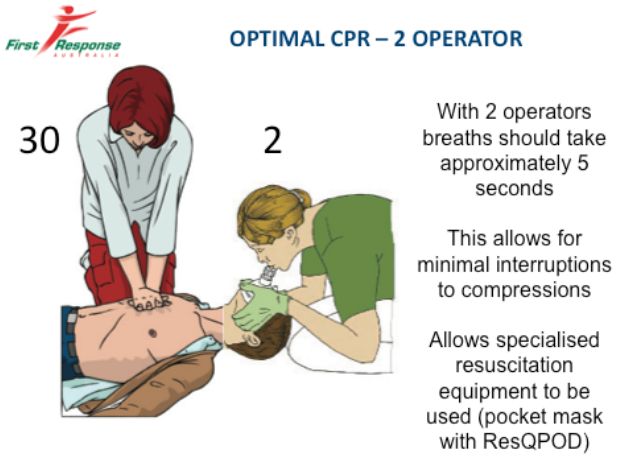
If
we now look at 2 rescuer
CPR we see a significant
change. Again, allowing
only 20 seconds to
complete 30
compressions, it now
only takes approximately
5 seconds to deliver the
2 breaths. Allowing for
the use of a
defibrillator every 2
minutes we end up with a
compression fraction
now, of approximately
70%.
It may
appear to some that this
is not a big difference,
but when we take into
account that
compressions are now
only being interrupted
by 5 seconds, this
results in better
forward blood flow reach
the heart and brain.
So, what
should be taught in a
standard "workplace CPR
program"?
Firstly,
for the witnessed adult
sudden cardiac arrest –
compression only CPR.
This is done whilst help
is being call for, a
defibrillator being
retrieved and calling
for more rescuers.
Next
should be the
application of a
defibrillator, followed
by 2 rescuer CPR. Note,
that ‘compression only
CPR’ has a compression
fraction of 90% plus.
In
summary; a quality CPR
program should include
the following CPR
instruction:
-
Adult
CPR – both 'compression
only' CPR and 2 rescuer
CPR
-
The
mandatory use of pocket
resuscitation masks as a
standard item for 2
rescuer CPR
-
Thorough training in the
use of AEDs
(defibrillators)
-
Standard CPR (30:2) for
infants and children
-
The
mandatory use of child
and infant manikins for
CPR training for these
age groups.
It is
concerning to note that
majority of training
organisations and their
trainers are suggesting
that child resuscitation
techniques are the same
as adult techniques –
this clearly is not the
case.
We also
should note, that across
the world the survival
rates are increasing
significantly when lay
rescuers do 'compression
only' CPR".
The
current Australian
guidelines suggest that
if the rescuer is
unwilling to do rescue
breaths, they should
continue with
uninterrupted
compressions.
There you
have it - we all should
be unwilling to do
rescue breaths unless we
have a fellow rescuer
assisting us with 2
rescuer CPR (and with a
pocket mask).
Watch the video
here
|